
Fertility Success Rate 2026: 50% Live Birth Under 35
- 3 days ago
- 6 min read

If you’re under 40 and considering fertility treatment, you need to understand the numbers that truly matter. Live birth rates per IVF cycle reach about 50% for women under 35 versus 21% for women aged 38-40, a striking difference that can dramatically influence your treatment timeline and decisions. Understanding true success metrics helps you choose treatments wisely, while AI and personalized care boost success rates and reduce treatment time, giving you a real advantage in your fertility journey.
Table of Contents
Key Takeaways
Point | Details |
Age dramatically impacts success | Women under 35 see nearly 50% live birth rates per cycle, dropping to 21% by ages 38-40. |
Success means live birth, not pregnancy | Clinical pregnancy rates mislead because they don’t account for miscarriage risk. |
AI improves outcomes by 15-20% | Advanced embryo scoring technologies significantly increase live birth rates over traditional methods. |
Expedited treatments maintain success | Rapid protocols reduce time and cost without compromising live birth rates. |
Clinic data requires careful interpretation | Patient demographics and reporting methods create wide variability in published success rates. |
What Is Fertility Success Rate? Definitions and Metrics
Fertility success rate sounds straightforward, but clinics and resources define it differently. The gold standard is live birth rate per assisted reproductive technology cycle, which counts only successful deliveries of a living baby. This metric matters most because it reflects your ultimate goal: bringing home a healthy child.
Many clinics report clinical pregnancy rates instead, which measure positive pregnancy tests or ultrasound detection of a gestational sac. These numbers look higher but don’t account for miscarriages occurring after initial confirmation. A clinical pregnancy rate of 60% might translate to only 45% live births after accounting for pregnancy losses.
International standards for reporting fertility data vary. The CDC maintains comprehensive statistics for U.S. clinics through the National ART Surveillance System, requiring all facilities to report outcomes. European registries use similar frameworks but may categorize age groups differently. When comparing success rates, verify you’re looking at live birth data per started cycle, not per embryo transfer, which excludes cycles that don’t reach transfer and inflates apparent success.
Key metrics to understand include:
Live birth rate per cycle started
Live birth rate per embryo transfer
Clinical pregnancy rate versus ongoing pregnancy rate
Cumulative success rates across multiple cycles
For reliable data, consult official CDC fertility success rate data that breaks down outcomes by age, diagnosis, and treatment type. These standardized reports let you compare clinics fairly and set realistic expectations for your personal situation.
Age-specific Fertility Success Rates for Women Under 40
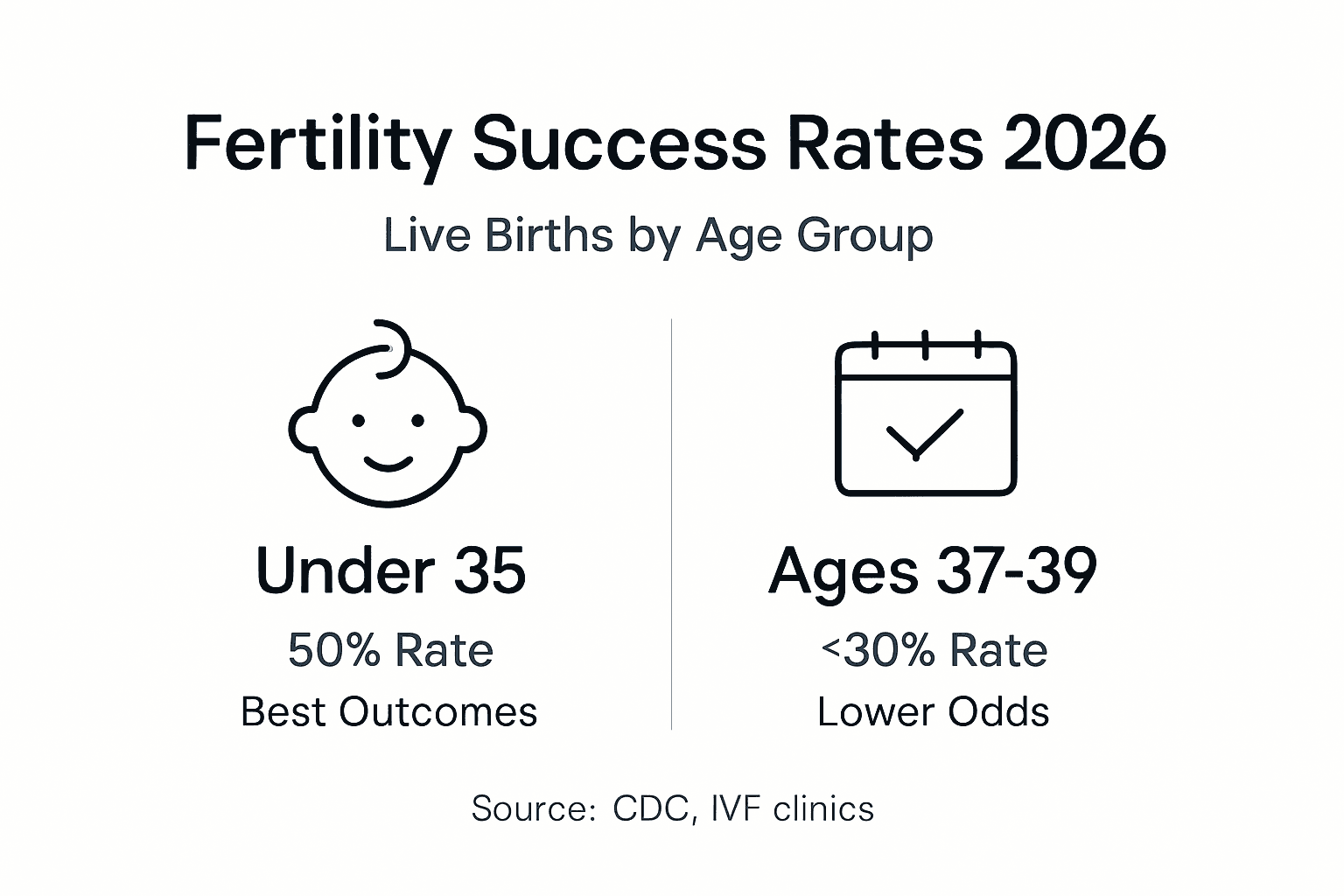
Your age is the single strongest predictor of fertility treatment success. Live birth rates reach about 50% for women under 35 and decline to 21% by age 38-40 per ART cycle, reflecting rapid changes in egg quality and quantity as you age. This decline isn’t linear. Success remains relatively stable through early thirties, then accelerates after 35.
Live birth rates drop below 30% by ages 37-39 due to diminished egg quality and quantity, making timing critical for women approaching this threshold. The biological mechanism behind this decline involves chromosomal abnormalities in eggs that increase with maternal age, leading to implantation failure or early pregnancy loss.
Age Group | Live Birth Rate Per Cycle | Key Considerations |
Under 35 | 50% | Highest success rates with fresh or frozen embryos |
35-37 | 38-42% | Moderate decline begins, still strong outcomes |
38-40 | 21-26% | Significant drop, genetic screening recommended |
Ovarian reserve plays an equally vital role in individual success probability. Two women at age 36 can have vastly different outcomes based on their remaining egg supply. Anti-Müllerian hormone (AMH) levels and antral follicle count (AFC) measure ovarian reserve, helping predict response to stimulation medications.
Women with good ovarian reserve at ages 38-40 often achieve success rates closer to younger age groups. Conversely, diminished ovarian reserve at 33 can create challenges typically associated with older ages. Testing these markers early provides crucial information for treatment planning.
Review detailed statistics at CDC ART success statistics and explore biological factors in this fertility journal’s age impact study00244-6/fulltext) to understand how your specific situation compares to national averages.
Key factors beyond age affecting success:
Body mass index (BMI) outside healthy range
Duration of infertility before seeking treatment
Male partner’s sperm quality
Previous pregnancy history
Presence of conditions like endometriosis or PCOS
Role of AI and Technology in Enhancing Success Rates
Artificial intelligence is revolutionizing fertility treatment by identifying viable embryos with unprecedented accuracy. AI-assisted embryo scoring improves live birth rates by 15-20% over traditional morphology-based methods, giving you a substantial advantage when selecting which embryo to transfer. Traditional embryo evaluation relies on visual assessment of appearance at specific time points, a subjective process prone to human error and limited information.
AI systems analyze thousands of images throughout embryo development, detecting subtle patterns invisible to the human eye. These algorithms learn from massive datasets of embryos with known outcomes, identifying characteristics that predict successful implantation and healthy pregnancy. The technology doesn’t replace embryologists but enhances their decision-making with data-driven insights.
Time-lapse imaging combined with AI enables continuous monitoring without disturbing embryos. The system captures images every few minutes, tracking division timing, fragmentation patterns, and morphological changes. AI processes this information to generate predictive scores, ranking embryos by viability.
How AI integration boosts your outcomes:
Reduces miscarriage rates by identifying chromosomally abnormal embryos
Decreases time to pregnancy by selecting optimal embryos first
Lowers costs by minimizing failed transfer cycles
Enables single embryo transfer while maintaining high success rates
Learn more about AI’s impact on fertility success and discover technology transforming IVF outcomes at leading clinics. The NCBI study on AI in embryology provides detailed research findings on these improvements.
Beyond embryo selection, AI personalizes medication protocols based on your hormonal response, predicting optimal dosing to maximize egg retrieval while minimizing ovarian hyperstimulation syndrome risk. Machine learning models analyze your treatment data in real-time, adjusting protocols mid-cycle when needed.
Pro Tip: Ask potential clinics whether they use AI-based embryo assessment and what specific improvements they’ve observed in their patient outcomes since implementation. Clinics using advanced technology should readily share this data.
Understanding why AI increases IVF success helps you evaluate whether a clinic’s technology investment translates to tangible benefits for patients like you.
Expedited Fertility Treatments and Their Impact on Success Rates
Traditional fertility treatment timelines stretch across months, requiring extensive preliminary testing before starting stimulation. Expedited protocols condense this process dramatically, sometimes beginning treatment within two weeks of initial consultation. You might worry that faster means compromising success, but evidence shows otherwise.
Expedited treatments maintain or improve success rates by eliminating unnecessary delays. Many standard protocols include tests that don’t change treatment decisions or wait periods between steps that aren’t medically required. Streamlined approaches focus testing on factors that genuinely impact protocol design, moving quickly to treatment while maintaining thorough evaluation of crucial factors.
Reduced treatment duration delivers multiple benefits:
Lower cumulative costs from fewer monitoring appointments and shorter medication timelines
Decreased emotional stress by shortening the anxious waiting period
Maintained ovarian reserve for women near critical age thresholds
Faster achievement of family building goals
Some clinics design protocols allowing cycle starts without waiting for specific menstrual cycle days, using medications to prepare your body regardless of natural timing. This flexibility eliminates month-long delays when initial consultation occurs at an inopportune cycle phase.
The fertility patient checklist outlines specific steps you can take to expedite your treatment start. Advanced embryo monitoring in fast-track fertility protocols ensures quality isn’t sacrificed for speed.
Pro Tip: Prepare for your first consultation by gathering medical records, completing preliminary bloodwork through your regular physician, and having your partner complete a semen analysis beforehand. This preparation can shave weeks off your treatment start date.
Expedited protocols work best for women under 40 with good ovarian reserve and no complex medical conditions requiring extensive preliminary treatment. If you fit this profile, rapid treatment pathways offer an efficient route to pregnancy without compromising your success odds.
Common Misconceptions About Fertility Success Rates
Misunderstanding success rate data leads many women to incorrect conclusions about their treatment prospects. The most pervasive misconception confuses pregnancy rates with live birth rates. Clinics sometimes prominently display pregnancy rates because they’re higher and sound more impressive, but pregnancy rates include early losses that never result in a baby.
A second major misunderstanding involves comparing raw success rates between clinics without considering patient populations. A clinic treating primarily complex cases or older patients will show lower success rates than one accepting only ideal candidates, even if the challenging-case clinic provides superior care. This comparison problem makes clinic shopping based solely on published rates unreliable.
Many women also believe all under-40 patients have similar success odds. As we’ve covered, the difference between 33 and 39 is dramatic. Even clinic categories like
Recommended
Comments